Docosahexaenoic acid (DHA) concentration in very low birth weight newborns receiving a fish-oil based fat emulsion from the first day of life. Preliminary clinical observation.
Stężenie kwasu dokozaheksaenowego (DHA) u wcześniaków z bardzo małą urodzeniową masą ciała, otrzymujących w żywieniu pozajelitowym od pierwszej doby życia emulsję tłuszczową opartą na oleju rybim. Wstępne obserwacje kliniczne
Dorota Pawlik1, Ryszard Lauterbach1, Maria Walczak2, Joanna Hurkała1
1Department of Neonatology
Head of Department: Professor R. Lauterbach MD.
Jagiellonian University, Collegium Medicum, Kraków, Poland
2Department of Pharmacokinetics and Physical Pharmacy
Head od Department: Professor J. Szymura-Oleksiak
Jageillonian University, Collegium Medicum, Kraków, Poland
Abstract
Background: Preterm infants are at increased risk for DHA deficiency because from 26th weeks of pregnancy until term, 80% of the brain this acid accrues in the fetus. Moreover, the main sources of lipids for preterm newborns are fat emulsions which do not contain DHA.
Aim: 1) to investigate the plasma DHA concentration in prematurely delivered newborns who are receiving a fish-oil emulsion in amount equal to one third of total daily intravenous lipid intake or soybean/olive oil fat emulsion from the first day of life. 2) to compare plasma DHA concentration, evaluated immediately after birth in prematurely born infants, with the respective data obtained in full term newborns.
Materials and methods: Twenty one preterm infants in the two groups: the study group n=12 (newborns fed parenterally with a partially replaced a soybean/olive oil emulsion with a fish-oil emulsion); the control group n=9 (newborn fed parenterally with a soybean/olive oil emulsion) comparable with regard to demographic and clinical characteristics. Determination of plasma and erythrocytes DHA concentrations in newborns was made using a high-performance liquid chromatography-mass spectrometry (LC-ESI/MS) method. Detection of parent ions with negative ionization mode, m/z 327,5 amu. Method validation was according to the ICH and FDA requirements.
Results: The mean values of plasma DHA level measured on the 7th, 14th, 21st, 28th day of life, were statistically significantly lower in the control group when compared with respective data obtained in the study group (7th day: 7.98 vs 42.4 μmol/L, p=0.0002; 14th day: 6.8 vs 21.14 μmol/l, p=0.000001; 21st day: 11.56 vs 19.1 μmol/L, p=0.035; 28th day: 11.4 vs 25.4 μmol/L, p=0.0004). The mean value of plasma DHA level in full-term newborns measured in the first hours of life was 164.7 μmol/L whereas in preterm neonates it reached 15.9 μmol/L (p=0.000001).
Conclusions: The administration of fish-oil-based fat emulsion as a component of total parenteral nutrition from the first day of life may alleviate a marked decrease in plasma DHA level observed in preterm infants within the first weeks after birth. Established method allows for routine determination of DNA concentrations in plasma erythrocytes of newborns.
Key words: docosahexaenoic acid, DHA, n-3 LCPUFA, VLBW infants, parenteral nutrition
Streszczenie
Wprowadzenie: Noworodki urodzone przedwcześnie obarczone są znacznym ryzykiem deficytu DHA gdyż ponad 80% zawartości tego kwasu w mózgu zostaje wbudowane w okresie pomiędzy 26 a 40 tygodniem ciąży. Z kolei emulsje tłuszczowe, które są najważniejszym źródłem lipidów dla wcześniaków w pierwszych tygodniach życia nie zawierają DHA, co nie pozwala na wyrównanie tego deficytu.
Cel badania: 1) ocena stężenia DHA w osoczu krwi u noworodków urodzonych przedwcześnie, żywionych parenteralnie bądź emulsją tłuszczową zawierającą olej rybi bądź też składającą się wyłącznie z tłuszczu sojowego i oliwkowego; 2) porównanie stężenia DHA w osoczu u wcześniaków i u noworodków donoszonych w pierwszej dobie życia.
Materiał i metodyka: 21 noworodków urodzonych przedwcześnie, podzielono na dwie grupy: grupa badana - 12 noworodków otrzymujących w żywieniu pozajelitowym emulsję tłuszczową zawierającą w składzie olej rybi oraz grupa kontrolna - 9 noworodków żywionych parenteralnie emulsją tłuszczową bez dodatku oleju rybiego. Grupy badane porównywalne pod względem wskaźników demograficznych i klinicznych. Oznaczenie stężenia DHA w osoczu i erytrocytach noworodków metodą wysokosprawnej chromatografii cieczowej sprzężonej z detekcją masową (LC-ESI/MS). Detekcja jonów macierzystych w trybie jonizacji ujemnej, m/z 327,5 amu. Walidacja metod zgodnie z wytycznymi ICH i FDA.
Wyniki: Średnie stężenie DHA w osoczu, oznaczone w 7, 14, 21 oraz w 28 dniu życia było statystycznie znamiennie niższe w grupie kontrolnej w porównaniu do analogicznych danych oznaczonych w grupie badanej (7 dzień: 7,98 vs 42,4 μmol/L, p=0,0002; 14 dzień: 6,8 vs 21,14 μmol/l, p=0,000001; 21 dzień: 11,56 vs 19,1 μmol/L, p=0,035; 28 dzień: 11,4 vs 25,4 μmol/L, p=0,0004). Średnie stężenie DHA w osoczu noworodków donoszonych, mierzone w pierwszych godzinach życia, wynosiło 164,7 μmol/L podczas gdy u wcześniaków osiągało wartość 15,9 μmol/L (p=0,000001).
Wnioski: Podaż emulsji tłuszczowej zawierającą dodatek oleju rybiego może zapobiegać znacznemu spadkowi stężenia DHA w pierwszych tygodniach po urodzeniu.
Słowa kluczowe: kwas dokozaheksaenowy, DHA, n-3 LCPUFA, żywienie parenteralne
INTRODUCTION
The fetal central nervous system undergoes rapid growth in the last trimester of pregnancy and docosahexaenoic acid (DHA) content in the brain increases significantly during this time (1, 2). Infants born prematurely are at risk for DHA insufficiency because they may not have benefited from the mother’s lipid stores (3). Within the first 1-2 weeks of life, the main sources of lipids for prematurely delivered, extremely low birth weight infants are most fat emulsions, which are rich in n-6 fatty acids and do not contain DHA. Consequently, supply of DHA is interrupted for a period of time, which is dependent on the immaturity of infants. Recently, in our observational study (4), carried out in small groups of patients, we found in infants, who were receiving a fish-oil based fat emulsion, either significantly lower risk of severe retinopathy or markedly decreased risk of cholestasis in comparison with newborns treated with conventional soybean/olive oil emulsion.
Therefore we performed an explorative study of a sample of preterm infants to investigate the plasma and erythrocytes DHA concentrations in those who were receiving a fish-oil emulsion in amount equal to one third of total daily intravenous lipid intake or soybean/olive oil fat emulsion from the first day of life. We hypothesized that those infants who were fed parenterally with a partially replaced a soybean/olive oil emulsion with a fish-oil emulsion would exhibit higher plasma and erythrocytes DHA contents during the first four weeks of life, when compared with patients receiving conventional soybean/ olive oil emulsion. The present study was also designed to compare plasma and erythrocytes DHA concentration, evaluated immediately after birth in prematurely born infants, with the respective data obtained in full term newborns.
PATIENTS AND METHODS
This study was approved by the Ethical Committee of the Jagiellonian University Medical College. Informed written consent was obtained from parents of all infants. Twenty one very low birth weight newborns, delivered prematurely before the 32nd week of gestation and admitted to the neonatal intensive care unit of the neonatal department of the Medical College of the Jagiellonian University in Kraków, who needed total parenteral nutrition were recruited for the study. Only patients without major congenital malformation or inborn metabolic errors and symptoms of congenital infection were enrolled. Twelve infants (the study group) were receiving a volume composition of lipid emulsions consisting of 50% of soybean/olive oil emulsion (20% Clinoleic, Baxter S.A.) and 50% of fish-oil emulsion (10% Omegaven, Fresenius Kabi AG). A source of lipid emulsion, administered parenterally in nine infants (the control group) was a 20% soybean/ olive oil emulsion (20% Clinoleic, Baxter). Both in the study and control group of infants, the lipid emulsions were administered from the first day of life as a continuous infusion 24 hours/day. The initial daily dose for infants with birth weight <1000 g was 0.5 g of lipids/kg body weight (0.15 g of Omegaven and 0.35 g of Clinoleic). Respectively, the initial dose for infants with birth weight >1000 g was 1.0 g of lipids/kg body weight (0.35 g of Omegaven and 0.65 g of Clinoleic). It was increased by 0.5-1.0 g of lipids/kg body weight every 24 hours to a maximum of 3.0-3.5 g of lipids/kg body weight/day (1.0 g-1.2 g of Omegaven and 2.0 g-2.3 g of Clinoleic). With regard to enteral feeding, infants in both groups were fed initially and advanced at 20 ml of breast milk (an average content of lipids ranges from 3.8 to 4.3 g/100 ml) and/or formula (Bebilon Nenatal Premium, Nutricia; 4.4 g of lipids per 100 ml) enriched with ω-3 LCPUFA/kg per day, according to feeding tolerance. The intravenous lipid infusion as a component of total parenteral nutrition was progressively replaced with enteral intake so as to maintain the total daily lipid dose at 3.0-3.5 g of lipids/kg body weight. The dosages and schedule of lipid administration were identical in both groups. The following data were collected in infants of both groups: birth weight, sex, gestational age, Apgar score and CRIB score.
For determination of plasma and erythrocytes DHA concentration, five blood samples were collected from prematurely born infants: in the first hour after birth, on the 7th , 14th , 21st and 28th day of life. Blood specimens were obtained by venipuncture or from an arterial catheter on the occasion of routine biochemical analysis. Also, for the comparison purposes, plasma and erythrocytes DHA concentrations were evaluated in blood samples, collected from 11 full-term newborns in the first hour after birth on the occasion of blood group determination. Plasma was separated from the blood within 30 minutes. Aliquots were stored at – 70°C until assayed.
Standard compounds of cis-4,7,10,13,16,19- docosahexaenoic acid (DHA), cis-4,7,10,13,16,19- docosahexaenoic acid methyl ester (internal standard, IS) and reagent grade ammonium acetate were purchased from Sigma (St. Louis, MO, USA). Gradient grade acetonitrile, water and ethanol were obtained from Merck (Darmstadt, Germany). Liquid chromatography was performed using an Agilent 1100 (Agilent Technologies, Waldbronn, Germany) LC system. Chromatographic separation was carried out with a Zorbax Eclipse XDB-C8 analytical column (150 mm x 4.5 mm, 5 μm, Agilent, Germany) set at 30°C. Analysis was performed in isocratic elution using a mixture of acetonitrile and water (80:20 v/v) with addition of 10 mmol ammonium acetate. The flow rate was set at 800 μL/min. The autosampler temperature was set at 4°C and a sample volume of 20 μL was injected into the analytical column for compound analysis. Mass spectrometric analyses were accomplished on an Applied Biosystems MDS Sciex (Concord, Ontario, Canada) API 2000 triple quadruple mass spectrometer equipped with an electro spray ionization interface and performed in the negative ionization mode. A standard polypropylene glycols solution (PPG 3000) was used for instrument tuning and mass calibration according to the Applied Biosystems manual. The mass spectrometer was operated with a dwell time of 200 ms, and a 5 ms delay between scans for each transition in the multiple ions monitoring mode (MI). To find the optimal parameters of the ion source and the ion path the mass spectrometer was tuned individually by direct infusion of each studied compound at a concentration of 5 μM at a flow rate of 10 μL/min using a Hamilton syringe pump (Hamilton, Reno, Nevada). The ion source parameters were as follows: ion spray voltage: 4500 V; nebulizer gas (gas 1): 20 psi; turbo gas (gas 2): 25 psi; temperature of the heated nebulizer (TEM): 400°C; curtain gas (CUR): 20 psi. The ion path parameters for DHA and IS were as follows: declustering potential (DP): 20V and 25V; focusing potential (FP): 200 V and 250 V; entrance potential (EP): 10V and 11V; electron multiplier (CEM): 2000 V; collision cell entrance potential (CEP): 10 V and 12 V, respectively. The mass spectrometer was operated at unit mass resolution in the multiple ions monitoring mode, monitoring the transition of the deprotonated molecular ions [M-H]- m/z 327.5 amu for DHA, and m/z 341.5 amu for the internal standard. The peak widths of the precursor ions were set to 0.7 full width half-height. The quantification analysis was performed via a peak area ratio of DHA to IS. Data acquisition and processing were accomplished using the Applied Biosystems Analyst version 1.4.2 software.
The stock solution of DHA was prepared at a concentration of 0.5 M in ethanol and was further diluted with ethanol to make working solutions at concentrations of 5000, 2500, 500, 50 and 5 μM. An internal standard working solution was prepared at a concentration of 146 μM with ethanol. All stock and working standards were stored at – 30°C pending analysis.
The precipitation of proteins to ethanol was a successful tool for DHA isolation from serum and erythrocyte. A 100 μL aliquot of the studied matrices were pipetted out into centrifuge tubes and the working internal standard solution (10 μL) and 1 mL of ethanol were added and then shaken for 20 min in vortex. After centrifugation at 3500 rpm for 15 min, the 0.5 mL of supernatants were transferred to other tubes and evaporated to dryness under a stream of nitrogen in a TurboVap LV (Caliper Life Science, Germany) and the sec residue was dissolved in 60 μL of ethanol, thereafter transferred to the inserts, and 20 μL was injected into the analytical column for DHA analysis (5).
Statistical analyses were performed with the use of Statistica for Windows (version 8.0) with probability <0.05 considered significant. The unpaired Student’s t-test was used to examine the differences between body weight, gestational age, Apgar score and CRIB values in the study and control group. The ANOVA for repeated measures was performed to compare the differences in plasma and erythrocytes DHA concentration. Post hoc comparisons of differences at specific days were then made with the Scheffe test.
RESULTS
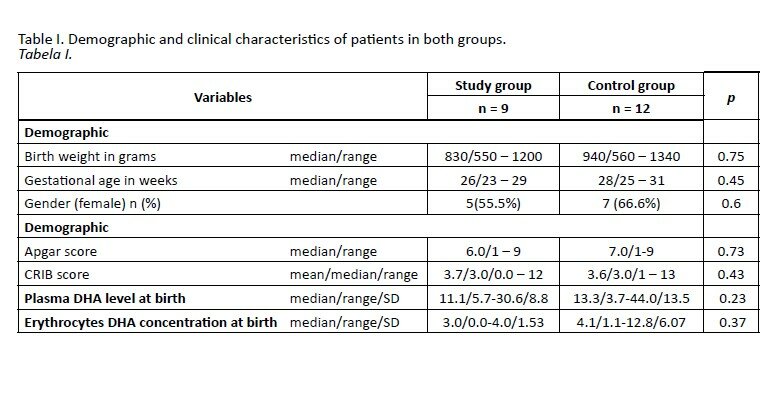
Table I shows that patients fed parenterally with two different fat emulsions were similar with regard to the birth weight, gestational age, Apgar score and CRIB. Also, either plasma or erythrocytes DHA concentrations, evaluated within the first hour after birth, were comparable in the two groups of newborns. The alterations in plasma DHA concentrations in both groups during the 4-weeks course of the study are shown in figure 1. There was a statistically significant decrease in plasma DHA concentration observed in the control group on the 7th day of the study (mean: 17.9 μmol/L vs mean: 7.98 μmol/L; p=0.044). However, the respective data concerning DHA levels in erythrocytes did not differ significantly (mean: 2.6 μmol/L vs 1.0 μmol/L; p=0.61). On the contrary, in the study group, a statistically significant increase in plasma and erythrocytes DHA concentrations was observed on the 7th day of life (plasma: mean: 13.3 μmol/L vs 42.4 μmol/L; p=0.0047; erythrocytes: mean: 2.46 μmol/l vs 38.1 μmol/L; p=0.0004). On the 14th day of life, the mean plasma DHA level in the control group was similar to data obtained on the 7th day (6.8 μmol/L vs 7.98 μmol/L). However, in the study group, there was marked decrease in plasma DHA concentration observed, but it did not reach the statistical significance (42.4 μmol/L vs 21.1 μmol/; p=0.12). The fluctuations of plasma DHA concentrations evaluated on the 21st, and 28th day of life in the two groups showed not statistically significant difference. Also, the direction of changes was similar in the study and the control group. Except of the initial data, the mean values of plasma DHA level measured on the 7th, 14th, 21st, 28th day of life, were statistically significantly lower in the control group when compared with respective data obtained in the study group (7th day: 7.98 vs 42.4 μmol/L, p=0.0002; 14th day: 6.8 vs 21.14 μmol/l, p=0.000001; 21st day: 11.56 vs 19.1 μmol/L, p=0.035; 28th day: 11.4 vs 25.4 μmol/L, p=0.0004). The determination of erythrocytes DHA concentration, in blood sample collected on 14th, 21st and 28th day of life was successful only in two infants in the control group and in three infants in the study group. Therefore, a further analysis of data concerning erythrocytes DHA concentration was not performed.
Comparisons between full-term newborns and preterm infants’ blood samples obtained within the first hour after birth, showed markedly higher, statistically significant, either plasma or erythrocytes DHA concentrations in patients delivered at term. The mean value of plasma DHA level in full-term newborns was 164.7 μmol/L (median: 167.0; ranges: 64.1-286.5; SD: 70.1) whereas in preterm neonates it reached 15.9 μmol/L (median: 11.1; range: 3.7-44.0; SD: 11.7). The difference was highly statistically significant (p=0.000001). Respective data concerning erythrocytes DHA concentration in blood samples obtained from full-term newborns were following: mean: 50.68 μmol/L; median: 33.9; range: 18.1-146.8; SD: 38.0. In prematurely delivered infants, erythrocyte DHA level was statistically significantly lower (p=0.006) with the mean value of 4.38 μmol/L; median: 3.1; range: 1.1-12.8 and SD: 4.2 μmol/L. Either in full-term newborns or preterm neonates, plasma DHA concentration did not correlate with respective data evaluated in erythrocytes (r=0.15).
DISCUSSION
The importance of lipids for growth and development of the central nervous system was already suggested by Widdowson in 1968 (6). During the last trimester of pregnancy, predominantly the long-chain polyunsaturated essential fatty acids (LCPUFAs) are transferred from the mother to the fetus (7). During this time and in the early neonatal period, rapid synthesis of brain tissue, with synaptogenesis and cellular differentiation has a special need for LC-PUFAs and DHA particularly. The recent researches stressed the importance of DHA, also for normal development of the glial cells (8). From 26 weeks of pregnancy until term, 80% of the brain DHA accrues in the fetus (9).
The results obtained in this study strongly suggest that infants born prematurely are at significant risk for DHA insufficiency. We found that in the first hour after birth, plasma and erythrocyte DHA concentrations in prematurely delivered infants were statistically significantly lower when compared to respective data obtained in full-term neonates. We also evaluated prospectively in preterm neonates possible associations between different (replaced partially a soybean/olive oil emulsion with a fish-oil emulsion or soybean/olive oil fat emulsion) lipids emulsions intake and plasma DHA patterns early after birth up to the age of 4 weeks of life. We showed that plasma DHA levels measured on the 7th, 14th, 21st, 28th day of life, were statistically significantly higher in the group of newborns, who were receiving a partially replaced a soybean/olive oil emulsion with a fish-oil emulsion, when compared with respective data obtained in the group of infants who were supplemented with soybean/ olive oil fat emulsion. It is widely accepted that preterm infants have very limited ability to synthesize DHA from the alpha-linoleic acid (ALA) (10) and moreover, within the first 1-2 weeks of life, the main sources of lipids for prematurely delivered newborns are fat emulsions, administered as components of total parenteral nutrition. These are mostly comprised of soybean oils, safflower, olive or MCT oils, and they do not contain DHA. In our previous study, describing the intravenous administration of partially replaced a soybean/olive oil emulsion with a fish-oil emulsion in very low birth weight infants from the first day of life, we found significantly lower risk of laser therapy in infants with retinopathy, who were receiving lipid emulsion containing DHA (4). It is important to remember that dosage and the schedule of both intravenous lipid emulsions administration were identical in our both studies. Therefore, we speculate that significantly increased plasma DHA level might influence the spontaneous regression of retinopathy in infants receiving fish-oil based lipid emulsion. As it was shown on fig. 1, the fluctuations of plasma DHA concentration evaluated on the 21st and 28th day of life, although did not show statistically significant differences, however, the visible tendency to increase was observed in the two groups. We suspect that a reason for this slight increase in plasma DHA level could be situation in which the intravenous lipid infusion as a component of total parenteral nutrition was progressively replaced with enteral intake of breast milk or enriched with DHA formula. However, the increased enteral intake of either breast milk or formula in infants in the control group was probably still insufficient so as to reach or even to approximate the values of plasma DHA concentration observed in newborns in the study group. According to our knowledge, this is the first study describing the evaluation of plasma and erythrocyte DHA concentration during the intravenous administration of different lipid emulsion: partially replaced a soybean/olive oil emulsion with a fish-oil emulsion or soybean/olive oil based fat emulsion, in very low birth weight infants from the first day of life. This study clearly showed that in the first hour after birth, plasma and erythrocyte DHA concentrations in prematurely delivered infants were statistically significantly lower when compared to respective data found in fullterm neonates. Whether we should increase the dosage of fish-oil based lipid emulsion as a component of total parenteral nutrition or to enrich formula so as to reach in preterm infants at 40th week of postconceptional age, the plasma DHA levels similar to those observed in term newborns, remains the question which could be explained in the future investigations.
CONCLUSIONS
The administration of fish-oil-based fat emulsion as a component of total parenteral nutrition from the first day of life may alleviate a marked decrease in plasma DHA level observed in preterm infants within the first weeks after birth. Established method allows for routine determination of DNA concentrations in plasma erythrocytes of newborns.
REFERENCES
1. Kidd P.M.: Omega-3 DHA and EPA for cognition, behavior and mood: clinical findings and structural-functional synergies with cell membrane phospholipids. Altern Med. Rev., 2007, 12, 207-227.
2. Farooqui A.A., Horrocks L.A., Farooqui T.: Modulation of inflammation in brain: a matter of fat. J. Neurochem., 2007, 101, 577-599.
3. Haggarty P.: Placental regulation of fatty acid delivery and its effect on fetal growth – a review. Placenta, 2002, 23, S28-38.
4. Pawlik D., Lauterbach R., Turyk E.: Fish-oil fat emulsion supplementation may reduce the risk of severe retinopathy in VLBW infants. Pediatrics, 2011, 127, 223-228.
5. Axelsen P.H., Murphy R.C.: Quantitative analysis of phospholipids containing arachidonate and docosahexaenate chains in microdissected regions of mouse brain. J. Lipid. Res., 2010, 51, 660-667.
6. Widdowson E.M., ed: Growth and composition of the fetus and newborn. Edited by: Assali NS. Academic Press, New York, NY; 1968.
7. ChampeilPotokar G., Chaumontet C., Guesnet P., Lavialle M., Denis I.: Docosahehaenoic acid (22:6n-3) enrichment of membrane phospholipids increases gap junction coupling capacity in cultured astrocytes. Eur. J. Neurosci., 2006, 24, 3084-3090.
8. Joardar A., Sen A.K., Das S.: Docosahexaenoic acid facilitates cell maturation and beta-adrenergic transmission in astrocytes. J. Lipid. Res., 2006, 47, 571-581.
9. Clandinin M.T., Chappell J.E., Leong S., Heim T., Swyer P.R., Chance G.W.: Intrauterine fatty acid accretion rates in human brain: implications for fatty acid requirements. Early Hum. Dev., 1980, 4, 121-129.
10. SanGiovanni J.P., ParraCabrera S., Colditz G.A., Berkey C.S., Dwyer J.T.: Meta-analysis of dietary essential fatty acids and long-chain polyunsaturated fatty acids as they relate to visual resolution acuity in healthy preterm infants. Pediatrics, 2000, 105, 1292-1298.
Adres do korespondencji / Address for correspondence:
Ryszard Lauterbach
Department of Neonatology
Jagiellonian University, Medical COllege
ul. Kopernika 23, 31-501 Kraków
Phone/fax: (48 22) 42-48-587
[email protected]