Acute appendicitis in children under 3 years of age. Diagnostic and therapeutic problems
Ostre zapalenie wyrostka robaczkowego u dzieci poniżej 3 roku życia. Trudności diagnostyczne i terapeutyczne
Maciej Bagłaj, Jolanta Rysiakiewicz, Konrad Rysiakiewicz
Department of Pediatric Surgery and Urology, Wroclaw Medical University, Wroclaw, Poland
Head: dr hab. D. Patkowski
Klinika Chirurgii i Urologii Dziecięcej, Akademia Medyczna we Wroclawiu
Kierownik: dr hab. D. Patkowski
Abstract
Aim: Analysis of diagnostic and therapeutic problems in acute appendicitis in children below 3 years of age.
Material and methods: The analysis was based on medical data of 53 children under 3 years of age, treated in our department for acute appendicitis in the years 1988-2008. Among 53 children, 29 (53.7%) were admitted directly to the surgical department and 24 (45.3%) were transferred from the regional pediatric department. In the period of 1 month before admission to the surgical department 13 patients (24.5%) were treated as outpatients due to acute respiratory or alimentary tract infection. On the basis of the data from the case histories, the most frequent symptoms and their duration were evaluated, as well as the clinical signs, intraoperative diagnosis and the postoperative course.
Results: The most frequent symptoms and clinical signs in this group of children were: abdominal pain, vomiting and fever, present in 83.0%, 75.5%, and 67.0% patients respectively. The mean time of the symptoms' duration was 3.6 days. The most frequently found physical signs on admission to the surgical ward were: abdominal pain on palpation, increased tonus of abdominal muscles and abdominal distension. On laparotomy gangrenous appendicitis was found in 49% of the children operated. In 24.5% of patients perforation of the appendix was confirmed. Further complications occurred in 9 children (16.9%). The average stay in hospital after the operation lasted 7.9 days.
Conclusions: 1. Acute appendicitis in small children is a diagnostic problem not only for primary health care doctors but also for experienced pediatricians and pediatric surgeons. 2. Early surgical consultation should be a standard procedure in small children with acute symptoms of various locations when there is accompaning abdominal pain, not reacting to conservative treatment. Surgical consultation is also indicated in children under 3 years of age with relapses of abdominal pain. 3. Clinical signs of appendicitis in children aged less than 3 years, may differ from those in older children due to changes in their immunological reactivity. This problem should be included in under-graduate and post-graduate medical studies.
Key words: overweight, obesity, children, gene polymorphism, FTO gene
Streszczenie
Cel: Analiza trudności diagnostycznych i terapeutycznych w ostrym zapaleniu wyrostka robaczkowego u dzieci poniżej 3 roku życia.
Materiały i metody: Materiał do analizy stanowiły dane z dokumentacji medycznej 53 dzieci w wieku poniżej trzeciego roku życia, leczonych w naszej klinice z powodu ostrego zapalenia wyrostka w latach 1988-2008. Spośród 53 dzieci – 29 (53,7%) zostało przyjęte bezpośrednio do oddziału chirurgicznego a 24 (45,3%) zostało przekazanych z rejonowego oddziału pediatrycznego. W okresie 1 miesiąca przed hospitalizacją w oddziale chirurgicznym 13 pacjentów (24,5%) było leczonych ambulatoryjnie z powodu ostrego stanu zapalnego układu oddechowego lub przewodu pokarmowego. Na podstawie dokumentacji oceniano najczęściej występujące objawy podmiotowe oraz czas ich trwania, objawy przedmiotowe, rozpoznania śródoperacyjne a także przebieg pooperacyjny.
Wyniki: Najczęściej odnotowanymi objawami podmiotowymi w grupie dzieci poddanych analizie były: ból brzucha, wymioty i gorączka stwierdzane odpowiednio u 83,0%, 75,5% oraz 67,0% pacjentów. Średni czas trwania objawów wynosił 3,6 dnia. Najczęściej stwierdzanymi objawami przedmiotowymi na podstawie badania fizykalnego w chwili przyjęcia do oddziału chirurgicznego były: bolesność uciskowa jamy brzusznej, wzmożone napięcie mięśni brzusznych oraz wzdęcie powłok brzucha. Śródoperacyjnie ustalono rozpoznanie zgorzelinowego zapalenia wyrostka u 49% dzieci. U 24,5% pacjentów stwierdzono perforację wyrostka robaczkowego. Powikłania odnotowano u 9 dzieci (16,9%), a średni okres pobytu w szpitalu po zabiegu wynosił 7,9 dnia.
Wnioski: 1. Ostre zapalenie wyrostka robaczkowego u małych dzieci stanowi trudny problem diagnostyczny, nie tylko dla lekarzy pierwszego kontaktu, ale także dla doświadczonych pediatrów i chirurgów dziecięcych. 2. Wczesna konsultacja chirurgiczna powinna być standardem postępowania u małych dzieci z ostrym stanem zapalnym różnych układów lub narządów przebiegających z dolegliwościami bólowymi brzucha i nie poddających się zastosowanemu leczeniu zachowawczemu. Na konsultację chirurgiczną powinny być kierowane dzieci poniżej 3 roku życia, u których doszło do ponownego wystąpienia dolegliwości bólowych po okresie wstępnej poprawy. 3. Objawy kliniczne zapalenia wyrostka robaczkowego u dzieci poniżej 3 roku życia mogą być odmienne niż u dzieci starszych ze względu na inną reaktywność organizmu, co powinno być przedmiotem szkolenia lekarzy.
Słowa kluczowe: ostre zapalenie wyrostka robaczkowego, bóle brzucha, dzieci poniżej 3 roku życia
INTRODUCTION
Acute appendicitis is the most frequent abdominal condition requiring emergency surgery in children. It may occur at any age but its incidence peaks at school age. Despite the advances in imaging medicine, the diagnosis of acute appendicitis remains based on clinical examination. A carefully taken history and physical examination allow reliable diagnosis in most cases (1, 2). Unfortunately this is very seldom seen in very young children. Acute inflammation of the appendix in this age group still remains a diagnostic dilemma for the clinician. Clinical symptoms and signs are not specific and frequently overlap with presentation of many other acute diseases occurring in the first years of life. Therefore, acute appendicitis in younger children is associated with a high rate of perforation of the appendix and greater morbidity than at an older age. There have been several reports of clinical aspects of acute appendicitis in younger children published in the medical literature to date. In most of them delay in the final diagnosis was emphasized as the main factor responsible for such a severe course of this disease (3, 4, 5).
We have undertaken a retrospective analysis of our own experience in the surgical management of children less than 3 years old with acute appendicitis in order to get an objective insight into the clinical presentation and outcome of treatment of this condition.
MATERIALS AND METHODS
Fifty three children aged 3 years or less operated on for acute appendicitis between 1988 and 2008 at the University Department of Pediatric Surgery in Wroclaw were selected from the hospital database and their case histories were reviewed. The final diagnosis was made in each case at laparotomy and confirmed histologically. The data regarding previous medical history prior to admission to the surgical unit, clinical symptoms and their duration, physical signs, the results of laboratory and imaging studies, surgical management, intraoperative findings, bacteriology, the postoperative course and the final outcome were extracted and analysed in detail. Changes in the appendix were arbitrarily graded as catarrhal, phlegmonous, gangrenous, gangrenous with perforation and periappendiceal abscess. There were 33 boys and 20 girls. The study group included 7 patients in the first year of life, one newborn and six infants. Ten patients were between 1 and 2 years old and 36 between 2 and 3 years. Thirteen children (24.5%) had received an oral antibiotic due to various acute diseases within one month prior to admission. Most of them had completed their treatment with temporary clinical improvement before the abdominal symptoms occurred or recurred. In nine of these patients the reason for treatment was respiratory infection, in a further two gastroenterocolitis and in two patients the precise cause could not be specified from their medical histories.
Twenty four children (45.2%) were initially admitted to the regional pediatric hospital before referral to the surgical department. The duration of hospitalization in the pediatric unit ranged from 1 to 7 days. All these children received oral or intravenous antibiotics. Twenty nine (53.7%) children were admitted directly to the surgical department. Fourteen of them were seen first by a local pediatrician or in the emergency department and immediately referred for surgical assessment.
RESULTS
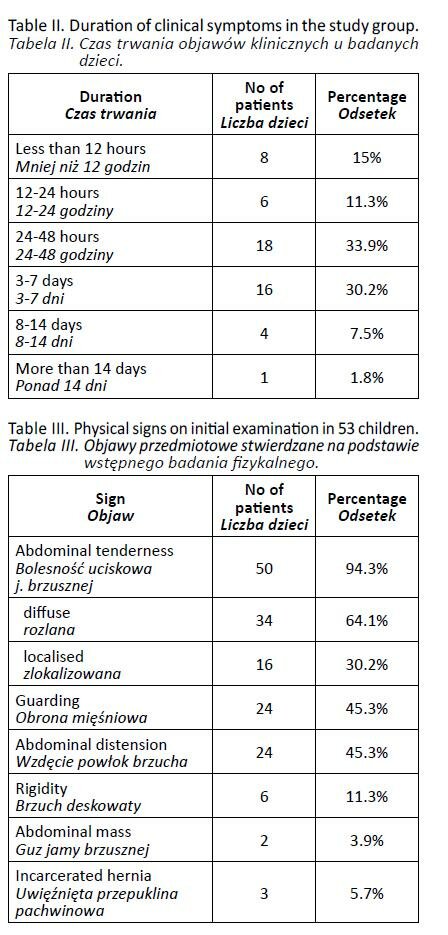
The principal clinical symptoms and their duration before admission to the surgical unit in the study group of children are presented in table I and table II respectively. The mean duration of the symptoms reported was 3.6 days and ranged between less than 12 hours and 21 days. Acute appendicitis was a referral or provisional clinical diagnosis made on admission in 20 children (37.7%). In 12 children it was non-specific acute abdominal disease and in the other 11 patients ileus was diagnosed. Suspicion of intussusception was raised in 6 children. Three children, aged 6 weeks, 3 months and 13 months respectively, were admitted due to incarcerated hernia. One patient was referred with the diagnosis of a pelvic mass.
The physical findings on clinical examination in the children studied are presented in table III. The highest white blood cell count (WBC) in the preoperative period ranged from 5600/mm to 28 500/mm3. In only one patient such data were missing. In 12 children (22.6%) WBC was less than 10 000/mm3 and in 33 (62.2%) it ranged between 10 000 and 20 000/mm. In a further 7 patients (13.2%) it was over 20 000/mm3.
Ten children did not have any imaging in the preoperative period and they were all treated before 1996.
Abdominal ultrasound (US), which has been available for emergency cases in our department from that year, was performed in 32 children (60.3%). In 9 patients it did not reveal significant pathology. Suspicion of acute appendicitis was raised on US in 11 patients. In three children an abdominal mass was noted. In single cases the US showed pericolonic infiltration, distended bowel loops, incarcerated inguinal hernia and thickened intestinal wall respectively. Two children had suspicion of intussusception on US. Abdominal US was the sole imaging modality in 15 children.
Twenty five patients (47.2%) had an abdominal x-ray taken preoperatively. Fourteen of them had both an x-ray and US. In 17 children it revealed distended small bowel loops locally with fluid levels. No significant abnormality or only intestinal distension were found in three cases. Poor aeration of the intestine and free abdominal gas indicating perforation were noted in single cases respectively. The last patient was a 5-day old newborn with isolated inflammation of the appendix and its perforation. In four children contrast enema was performed. In two of them the small bowel could not be visualized. In the other two it excluded the initial suspicion of intussusception.
Forty one children (77.3%) were operated on the day of admission. Nine patients (16.9%) underwent surgery on the second day of hospitalization in the surgical unit and in 3 children (5.6%) operative treatment was delayed until the third day after admission. Forty patients were subjected to open laparotomy and in a further 10, laparoscopic procedure was performed. In three children with incarcerated hernia, formal repair was undertaken with intestinal manipulation and appendicectomy performed via inguinal approach. Intraoperative findings were consistent with gangrenous appendicitis in 26 children (49%), including 13 with perforation (24.5%). Nine children (16.9%) had catarrhal inflammation while in a further 15 patients (28.3%) phlegmonous appendicitis was noted. Three children had periappendiceal abscess found on laparotomy and required drainage only. In the postoperative period all patients received intravenous antibiotics. Five children required referral to the Paediatric Intensive Care Unit due to their poor general condition in the immediate postoperative period. Postoperative complications were noted in 9 children (16.9%). In three of them prolonged paralytic ileus was noted. In 3 other children intraabdominal abscess occurred. In all of them resolution of the inflammation was obtained with conservative therapy. One child required early re-laparotomy due to an adhesive obstruction. Wound infection was noted in 2 children. The duration of hospitalization in the surgical department ranged from 5 to 21 days (mean 7.9 days). All the children were discharged home.
In 26 children (49%) the results of microbiological studies were available for analysis. In only one child the culture did not yield any growth of bacteria. In children with positive bacteriology, one strain was identified in 8 of them, while in 17 at least 2 strains were cultured. Altogether 19 various strains were identified in the study group. Among them, Escherichia coli was the most frequent strain found in 14 children. Peptostreptococcus and Bacteroides fragilis were identified in 5 cases each. Four strains: Micrococcus, Kliebsiella pneumonia, Kliebsiella oxytoca and Pseudomonas occurred in 2 patients each. Twelve strains were noted only in a single case.
DISCUSSION
Acute appendicitis must be considered in the differential diagnosis of every school-age child presenting with acute abdominal complaints. Such a common occurrence is not typical for younger children. The lower the age of the patient, the less probable is the inflammation of the appendix. The epidemiology of acute appendicitis in very young children is well reflected by the low number of patients reported from various pediatric centres worldwide. This number, when calculated for children less than 3 years of age, ranges from less than one to 11 per year per department (4, 6, 7, 8, 9).
There are several factors dictating the age of 3 years and less as a selection criterion for a clinical study. Epidemiological aspects have been mentioned above. This is a group of children not able in most instances to express their complaints verbally and medical history is based exclusively on the description given by the parents or their caregivers. On the other hand, there is no organ or system-specific symptomatology and many acute conditions at this age may present a similar, frequently overlapping, clinical picture. Moreover, physical examination of the abdomen, the cornerstone for clinical diagnosis of acute appendicitis in older children, may be very difficult and thus unreliable in a sick very young child. All these factors contribute to the fact that diagnosis of acute appendicitis in the first years of life may be a diagnostic dilemma for the clinician. It has been uniformly labelled as a condition associated with diagnostic delay, a severe clinical course and high rate of complications (7, 10, 11). It may provoke the question whether such differences should be attributed to the very young child as a different patient not able to present with a common clinical picture or whether acute appendicitis in this age group should be regarded as a different disease due to age-related anatomical and physiological factors. Among 53 children in our series, 24.5% had been treated with antibiotics before surgical management. On including those admitted initially to the local pediatric hospital prior to referral to the surgical department this figure rises to nearly 70%. Allo et al mentioned that 52% of children in their series had been treated for acute illness before admission to the surgical unit and the mean delay in the final diagnosis of acute appendicitis was 3 days (7). Similar data were cited by Horwitz et al. who found the mean delay between the onset of symptoms and presentation to a physician of 4.3 days (8). In both reports their authors emphasized a high rate of misdiagnosis made by a physician initially reviewing the very young child, of 67% and 58% respectively. In the group of 155 preschool children with acute appendicitis reported by Graham et al. 57% of them had been treated with antibiotics for 6 to 130 hours, earlier in their illness (11). Sakellaris et al. reported that the children aged 4 and less had a mean duration of symptoms of 97 hours, compared to 55 hours in those of 4 and 5 years of age (4). Considering all these clinical reports, it should be stressed that more than 50% of children less than 3 years old operated on for acute appendicitis had been seen by a physician early in the course of their disease. Most of them were treated with antibiotics. It may be speculated on whether this should be regarded as the true onset of acute abdominal condition in this subset of patients. Such is the trend in the literature dealing with this subject blaming the physicians for not diagnosing a true pathology correcth and causing unnecessary delay. This view might be correct assuming that the young child suffers from acute inflammation of the appendix from the very onset of his or her disease regardless of the initial symptoms. This hypothesis finds its support in the fact that there is a direct relation between the duration of symptoms and the grade of inflammation of the appendix (6, 9, 12). On the other hand it might well be that the initial disease refers to the other organ or system with variable clinical presentation including more or less expressed abdominal complaints. This first illness might act as a triggering factor for inflammation of the appendix. Treatment with antibiotics might only delay the presentation of appendicitis. Such a two-step hypothesis would not be negated by the high rate of perforated appendicitis in this age group. Taking into consideration that the immature anatomical structure of the appendix in small children with a significantly thinner wall than in older children and the lack of an adequate omental barrier might help to support the notion of the more rapid progress of inflammation in younger patients. So according to this alternative hypothesis, it is not the duration of symptoms but a more rapid progress of inflammatory lesions across the appendiceal wall that is responsible for the more severe course.
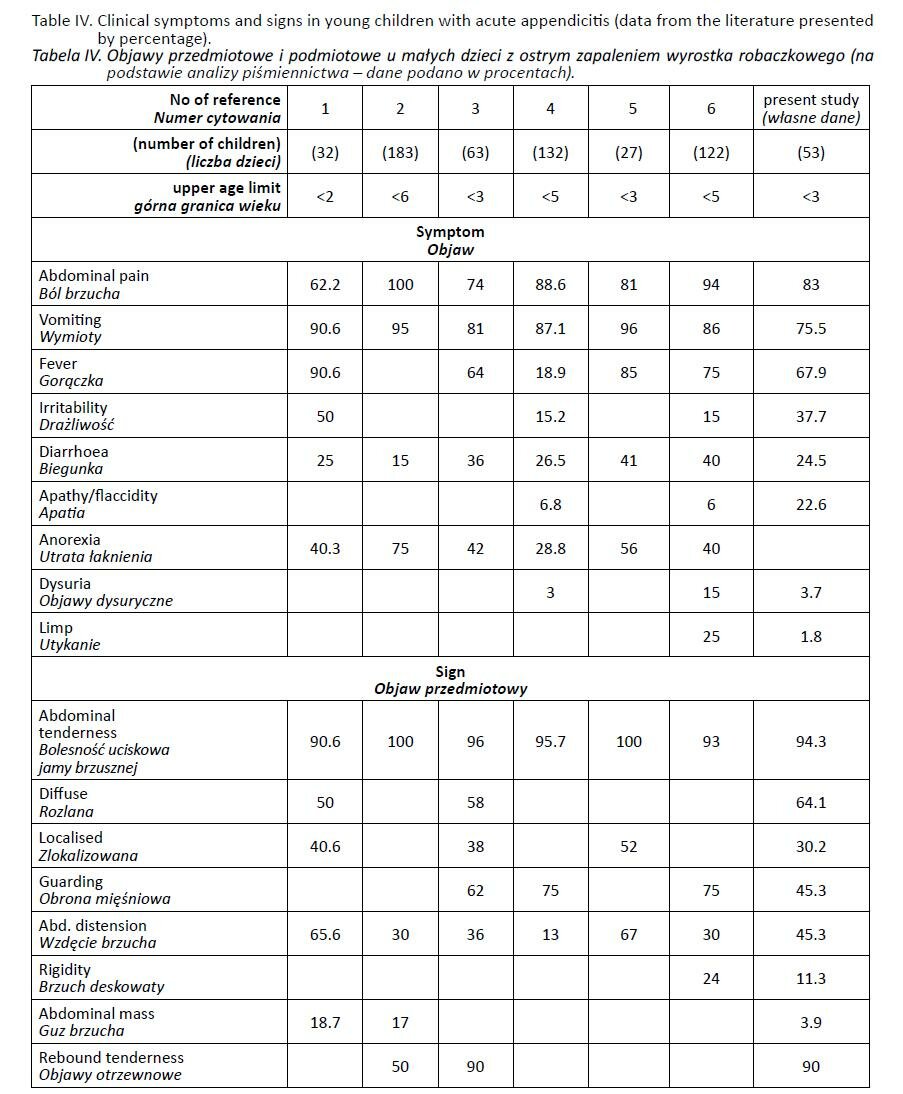
Acute appendicitis in very young children does not present with a uniform clinical pattern. Although abdominal pain, vomiting and fever are still the cardinal symptoms, they are frequently accompanied by general symptoms obscuring the clinical picture or shifting the attention of the parents or physician to other illnesses. If we consider abdominal pain alone, it is not reported in all patients as a dominant feature. On the other hand it is very difficult to assess abdominal discomfort in a child not able to define his or her complaints verbally. Instead, these children may present with irritability as a principal symptom. We feel that in many young children, irritability, especially when coupled with vomiting, is taken indirectly as a proof of abdominal pain. In table IV we have summarized the symptoms and signs in young children with acute appendicitis reported in the literature. Despite the limited number of patients collected, the differences between the contributing authors are surprising. To some extent they result from including older children of preschool age as well (4, 6, 11). But even focusing on the studies referring to the youngest children less than 3 years of age, it may be difficult to establish the common clinical picture. Such important symptoms as apathy or irritability are not reported by some authors (7, 8, 9). Conversely, anorexia is reported by many of them as a frequent symptom, although we feel that any vomiting child of 3 years of age or less will always be presenting with loss of appetite or generally with anorexia. Fever was found in 67.9% of our patients. Similar data were presented by Horwitz et al. (8). Earlier treatment with antibiotics in many of these patients might explain such a febrile course of the disease. Taking into account the variability and long duration of symptoms in these children it is not surprising that they were referred to the surgical units with various clinical diagnoses. In our series, only 37% of the patients were admitted with a provisional diagnosis of acute appendicitis. The high rate of incorrect referral diagnosis was stressed uniformly by most authors presenting their experience (4, 5, 6, 9). Analyzing the collective review of physical signs in children reported from various surgical centres one must emphasize the significant differences again. Abdominal tenderness is almost uniformly noted by all authors. We noted that in nearly 2/3 of our patients generalized diffuse tenderness was present, while a localized tenderness on initial examination was found in 30% of the reviewed children. In the series of 27 children Allo et el. reported localized tenderness at presentation in 50% of them but surprisingly all of them had perforated appendicitis (7). A similar discrepancy between clinical signs and final pathology can be noted in the report by Hortwitz et al. (8). Guarding, such a typical physical sign for an older child, was reported with variable frequency by the authors. The same holds true in the case of abdominal distension ranging from 13% to 67% in the reported series (6, 7, 8). Analysing this collective summary of physical symptoms in children, two facts must be emphasized. Firstly, all were reported by pediatric surgeons after a considerably long course of the disease in most of them and secondly, at least half of these patients had perforated appendicitis noted at laparotomy. Taking only the surgical reports into consideration, it is therefore impossible to define the natural history of acute appendicitis in very young children.
There is no laboratory investigation which would be helpful in making a diagnosis more probable in the preoperative period. Well known markers of inflammation, including leukocytosis, might show variable values and hence are not very reliable. In our material 22.6% of the children did present with WBC less than 10 000/mm. Similar data were also reported by other authors (4, 6, 7). It must be stressed, however, that more than 60% of our patients had been treated with antibiotics before admission to the surgical unit. We could not assess the initial values of WBC in many of these patients. Interesting data was presented by Lin et al. reporting a series of 7 children aged less than 1 year with acute appendicitis. In 5 of them WBC was less than 5000/mm despite having a gangrenous appendicitis (10). Such observation once again emphasizes the differences between small children and school-age patients. In our series there was also no significant correlation between the pathological grade of appendicitis and WBC.
It is beyond doubt that the clinical examination of a sick young child may be a challenge even for an experienced surgeon. An objective assessment may only be possible when the child settles down or falls asleep. Therefore, in cases of any diagnostic doubt, formal admission and repeated abdominal examination seems the best policy (4). Obtaining the diagnosis on clinical grounds might be very difficult and therefore a high number of young children with appendicitis had imaging studies performed preoperatively. In our material, only ten children (18.9%) did not have any imaging. In the series reported by Horwitz et al. 82.5% of patients had an abdominal radiograph and 38% of them had more than one imaging study (8). Allo et al. noted that an abdominal x-ray was performed in 75% of patients analysed (7). All the children reported by Grosfeld et al. had abdominal radiography (9). Such a frequent use of imaging modalities is a clear argument that diagnosis of acute appendicitis in a very young patient is not easy even for paediatric surgeons. Therefore, in our opinion ascribing the diagnostic delay to the primary care physician is truly unfair. The principal purpose of imaging is usually to exclude other potentially surgical conditions, because acute appendicitis is not of primary concern. In the infants and younger children intussusception must be seriously taken into consideration, hence such a significant number of them had an ultrasound scan and contrast enema performed (2, 7).
There is a significant variability in the use of imaging studies in very young children affected by acute appendicitis. In our very limited experience, the US was a study of better specifity and accuracy, especially in the most recent cases. There is no specific radiological pattern of acute appendicitis, although in nearly 70% of those who had abdominal x-ray focal distension of the small bowel loops with fluid levels were noted. Very similar results regarding x-ray findings were reported by Grosfeld et al., who noted ileus pattern in 78% of their patients (9). Small bowel obstruction on abdominal radiograph was demonstrated in 66.7 % of the children reported by Allo et al. (7). The role of imaging studies in the young children has not been thoroughly discussed in the literature and some authors did not even mention the aspects of diagnostic management in their reports (4, 6). In older children some authors advocate computed tomography in cases of atypical clinical presentation (13). This issue undoubtedly deserves further clinical studies also in very young children.
Discussing diagnostic delay in young children with acute appendicitis, one additional factor must be frankly explained, namely the delay in the undertaking of operative management. We were able to find that in more than 22% of the patients operative treatment had been delayed for one or even two days. Grosfeld et al. noted a mean delay of 16 hours in the group of children less that 2 years of age (9). Other authors did not discuss this aspect but it cannot be omitted in an objective presentation of acute appendictitis in young children. We feel obliged to stress that such a “surgical” delay, a phenomenon very seldom encountered in cases of acute appendicitis in older children, might result from the difficulty of making a final diagnosis, the necessity of clinical observation of the patient with repeated physical examination or the time consumed for additional imaging studies.
The true nature of acute appendicitis in very young children is best reflected by a high incidence of a complicated form of appendiceal inflammation with a high rate of perforation ranging from 45% to 100% (4, 6, 7, 8). In our material it was 24.5%, but when gangrenous appendicitis is taken into consideration this rate increases to 49. Similarly to perforated appendicitis, the incidence of periappendiceal abscess during the first 3 years of life is much higher than in older counterparts (6, 7). Such a high fraction of perforation is the principal cause for a high rate of postoperative complication and postoperative morbidity. In our material the mean hospital stay exceeded 7 days and postoperative complication occurred in 16.9% of patients. Similar high postoperative morbidity in very young children subjected to operative treatment is reported uniformly in the literature (5, 7, 9). Analysis of bacteriological data obtained in our patients does not indicate that inflammation of the appendix in small children might be linked to unusual flora. Escherichia colli was the most frequent strain reported. Comparing these results with those obtained in older children by other authors, it does not seem that different clinical course and higher complication rate of appendicitis in small patients might find its explanation in different bacteria involved in the inflammation (2, 14). This issue has been seldom discussed by other authors presenting their series of small children. Lin and Lee reported a very high inicidence of Pseudomonax aeruginosa of 85.7% among infants less than one year of age (10). We could not confirm this observation in our material but it undoubtedly deserves further investigation in the youngest children with acute appendicitis.
In summary, reviewing our own material and the experience of other authors, it appears that despite the significant advances in modern medicine, acute appendicitis in very young children still presents a clinical challenge. It may present with various clinical patterns, very often mimicking other acute diseases. There is no diagnostic modality which can help the clinician at the early stages of appendicitis. A delay in diagnosis seems to be a pertinent attribute. Claiming that a high index of suspicion might reduce the morbidity of acute appendicitis in very young children, according to our observation, sounds like simplification of the problem (6). We represent the opinion that delay in the final diagnosis during the first years of life is multifactorial and cannot be attributed to primary care physicians only. It is not that surgeons are able to diagnose this entity promptly and only late referral to surgical units results in a high rate of perforation. A thorough analysis of clinical aspects does not give convincing evidence that appendiceal inflammation in very young children follows the same clinical course as that of older children. It cannot be excluded that the more rapid progress of inflammation involving the appendix leads to a high rate of very advanced pathology and preceding diseases of respiratory or gastrointestinal tracts with abdominal symptoms should be regarded not as the onset of intraabdominal pathology but rather as a predisposing factor. Regardless of the true natural history of acute appendicitis, the problem how to diagnose this disease promptly and effectively in a very young child remains open. An early surgical consultation of a child not responding to treatment of acute illness presenting with abdominal complaints or with recurrent symptoms after various periods of improvement sounds like the only reasonable advice to every physician. The decision about operative intervention in children with evident clinical signs of intraabdominal pathology seems to be obvious and can be supported by an ultrasound scan or abdominal x-ray. In children with less advanced pathology and thus less clear clinical picture, such a decision is very difficult. We hypothesize that early laparoscopy in these patients might serve its use as a reliable diagnostic and therapeutic tool. The question who and when should be subjected to such a procedure seems to be an ideal subject for prospective multiinstitutional research study.
CONCLUSIONS
1. Acute appendicitis in small children is a diagnostic problem not only for primary health doctors but also for experienced paediatricians and pediatric surgeons.
2. Early surgical consultation should be a standard procedure in small children with acute symptoms of various locations when there is accompaning abdominal pain, not reacting to conservative treatment. Surgical consultation is also indicated in children under 3 years with relapses of abdominal pain
3. Clinical signs of appendicitis in children aged less than 3 years may differ from those in older children due to changes in their immunological reactivity. This problem should be included in under-graduate and post-graduate medical studies.
REFERENCES
1. Reynolds S.: Missed appendicitis in a pediatric emergency department . Pediatr Emerg Care 1993, 9, 1-3.
2. Davenport M.: Acute abdominal pain in children. BMJ, 1996, 312, 498-501.
3. Daum R., Hecker W., Tessmar J.: Appendicitis perforata im Sauglings- und Kinderalter. Med Munch Wochenschrifft 1969, 111, 2193-2197.
4. Sakellaris G., Tilemis S., Charissis G.: Acute appendicitis in preschool-age children. Eur. J. Pediatr. 2005, 164, 80-83.
5. Bagłaj M., Czernik J., Szewczyk K., Płaksej R.: Ostre zapalenie wyrostka robaczkowego u niemowląt i małych dzieci. Pol. Przegl. Chir. 2000, 11, 977-990.
6. Surana R., Quinn F., Puri P.: Appendicitis in preschool children. Pediatr. Surg. Int. 1995, 10, 68-70.
7. Allo J., Gerstle T., Shilyansky J., Ein S.: Appendicitis in children less than 3 years of age: A 28-year review. Pediatr. Surg. Int. 2004, 19, 777-779.
8. Horwitz J., Gursoy M., Jaksic T., Lally K.: Importance of diarrhoea as a presenting symptom of appendicitis in very young children. Am. J. Surg. 1997, 173, 80-82.
9. Grosfel D.J., Weinberger M., Clathowrthy W.: Acute appendicitis in the first two years of life. J. Pediatr. Surg. 1973, 8, 285- 293.
10. Lin Y., Lee C.: Appendictis in infancy. Pediatr. Surg. Int. 2003, 19, 1-3.
11. Grahan J., Pokorny W., Harberg F.: Acute appendicitis in preschool age children. Am. J. Surg. 1980, 139, 247-250.
12. Bratu I., Martens P., Leslie W., Dik N., Chateau D., Katz D.: Pediatric appendicitis rupture rate: disparities despite universal health care. J. Pediatr. Surg. 2008, 43, 1964- 1969.
13. Horton M., Counter S., Florence M., Hart M.: A prospective trial of computed tomography and ultrasonography for diagnosing appendicitis in the atypical patient. Am. J. Surg. 2000, 179, 379-381.
14. Mosdell D., Morris S., Fry D.: Peritoneal cultures and antibiotic therapy in pediatric perforated appendicitis. Am. J. Surg. 1994, 167, 313-316.
Adres do korespondencji:
Maciej Bagłaj
Department of Pediatric Surgery and Urology,
Wroclaw Medical University
M. Sklodowska-Curie 52, 50-367 Wroclaw, Poland
tel. 0048-71-7703001, fax: 0048-71-7703009
[email protected]